
Introduction: A Conversation That's Missing from Every CKD Appointment
If you've ever sat in a nephrologist's office, you know the routine.
You get the list:
- Watch your potassium.
- Watch your phosphorus.
- Watch your sodium.
- Watch your protein.
Four minerals to watch, four foods to pull from the plate — and that's usually where the dietary conversation ends.
But there is a fifth mineral that often gets less attention — even though a growing body of kidney and cardiovascular research keeps pointing to the same question:
Could low magnesium be contributing to worse vascular, metabolic, and kidney outcomes in some CKD patients?
In my interview on The Michael D Show about my book Your Kidneys Can Heal, I keep coming back to one point: why so many CKD patients plateau — or decline — even when they "do everything right."
The blind spots in kidney care are not always exotic. Sometimes they are basic factors that deserve a closer look.
Magnesium is one of those basics.
"We obsess about what's too high in our patients. We rarely ask what is too low."
Watch the full interview:
This article explains why magnesium matters for kidney patients, why some CKD patients become depleted, why a normal serum magnesium does not always tell the whole story, which medications raise risk, how to discuss safe correction with your clinician, and how food and lifestyle choices can support long-term magnesium status.
Why Nephrology Got So Focused on Potassium (and What It Costs Patients)
There is a reason potassium gets all the attention.
When kidneys lose the ability to excrete potassium, blood levels can climb fast. Hyperkalemia — high potassium — can trigger:
- Muscle weakness
- Dangerous heart rhythms
- Cardiac arrest
So nephrologists are trained, correctly, to be aggressive about preventing it. That's where the familiar restrictions come from — the bananas and oranges you give up, the lists you memorize, the whole idea of a "renal diet."
But somewhere in the focus on what your kidneys can't get rid of, the conversation about what some patients may be losing or under-consuming can disappear.
Magnesium belongs in that second conversation.
Studies report very different rates of low magnesium in CKD depending on stage, diabetes status, dialysis status, medications, diet, and how magnesium is measured. At the same time, advanced CKD can also increase the risk of high magnesium if intake or medications add too much. In other words: magnesium status in CKD is important, but it is not something to guess.
That matters because magnesium is doing a lot of work behind the scenes.
What Magnesium Actually Does for Your Kidneys
Magnesium does far more than most people realize. It's a foundational cofactor in over 600 enzymatic reactions in the human body, and the kidney depends on it for some of its most basic functions.
Here is what the research suggests:
1. It May Help Protect Against Vascular Calcification
This may be the single biggest reason magnesium matters in CKD.
When kidneys lose function, calcium and phosphorus balance becomes deranged. Calcium starts to deposit where it shouldn't — in blood vessels, in heart valves, in the kidneys themselves.
This process — vascular calcification — is one of the main reasons CKD patients have such high rates of heart disease and cardiovascular death.
Magnesium appears to oppose several steps in that process.
- It competes with calcium at deposition sites
- It stabilizes calcification-inhibiting proteins like fetuin-A
- It reduces the upstream signaling that drives the process
Observational studies repeatedly link lower magnesium with more vascular calcification and worse cardiovascular outcomes in CKD. Clinical trials are more mixed: magnesium supplementation can raise magnesium levels and may improve some vascular markers, but meta-analyses have not consistently shown reduced vascular calcification scores. That makes magnesium important, but not a magic bullet.
2. It Lowers Inflammation and Oxidative Stress
Like L-carnosine, magnesium is part of the body's anti-inflammatory toolkit.
Low magnesium has been linked to:
- Elevated CRP and IL-6
- Increased oxidative stress markers
- Endothelial dysfunction
- Reduced glutathione activity (your master antioxidant)
In CKD — where inflammation often contributes to progression — low magnesium may add another layer of stress.
3. It Supports Healthy Blood Pressure
Magnesium helps blood vessels relax. It's involved in:
- Nitric oxide signaling
- Smooth muscle function
- Aldosterone regulation
- Renin-angiotensin balance
For kidney patients — where blood pressure is both a cause and consequence of disease — correcting a true deficiency may support the broader blood pressure plan. It should not replace prescribed medication.
4. It Improves Insulin Sensitivity
This carries real weight for the millions of CKD patients who also have diabetes or metabolic syndrome.
Magnesium is required for normal insulin signaling. Low magnesium can worsen insulin resistance, which can make blood sugar control harder — an important issue for diabetic kidney disease.
It is one of the more plausible mechanistic links in metabolic kidney disease.
5. It Reduces Proteinuria in Some CKD Populations
Some studies have linked better magnesium status or repletion with lower albuminuria in selected populations, but this is not yet a universal treatment claim.
This is the same biology L-carnosine and SGLT2 inhibitors are influencing. Magnesium reaches it from a different angle.
6. It Plays a Role in Calming the Nervous System
CKD patients are chronically stressed — biologically and emotionally. Magnesium is required for:
- GABA signaling
- Sleep regulation
- Stress hormone modulation
- Muscle relaxation
Leg cramps, restless sleep, anxiety, and tension headaches can have many causes in CKD. When magnesium is low, it can be one correctable contributor.
Why CKD Patients Are Systematically Depleted
This is the part that frustrates me most.
Some patients with kidney disease become low in magnesium because diet, medications, diabetes, and tubular dysfunction can all work against magnesium status.
The "Renal Diet" Restricts Magnesium-Rich Foods
The foods richest in magnesium are the same ones that get restricted in conventional CKD diets because they are also high in potassium or phosphorus:
- Leafy greens (spinach, Swiss chard)
- Nuts and seeds (especially pumpkin and chia)
- Legumes
- Whole grains
- Dark chocolate
- Avocado
When most of these foods disappear without individualized replacement, magnesium intake can fall.
Common Kidney-Patient Medications Strip Magnesium
Several medications used in nephrology and primary care can raise the risk of low magnesium:
- Proton pump inhibitors (PPIs) — omeprazole, esomeprazole, pantoprazole. The FDA has issued formal warnings about PPI-induced hypomagnesemia after long-term use.
- Loop diuretics — furosemide, torsemide, bumetanide. Powerful magnesium wasters in the urine.
- Thiazide diuretics — hydrochlorothiazide, chlorthalidone.
- Aminoglycoside antibiotics — gentamicin, tobramycin.
- Cisplatin and other chemotherapy agents.
- Metformin — modest but real effect over time.
If your medication list contains a PPI plus a diuretic, you have a stronger reason to ask whether magnesium should be checked.
Diabetes and Insulin Resistance Increase Losses
People with diabetes lose more magnesium in their urine, especially when blood sugar is elevated. Glucose spills into urine and drags magnesium with it.
Given how many CKD patients are diabetic, this can be a meaningful driver of low magnesium.
Stress and Chronic Inflammation Burn Through It
Stress hormones can increase magnesium excretion, and chronic inflammation may shift magnesium needs. This is one more reason symptoms, diet, medications, and labs need to be interpreted together.
The standard "magnesium level" your doctor orders is useful, but it has limits.
Why Standard Magnesium Blood Tests Can Miss Part of the Problem
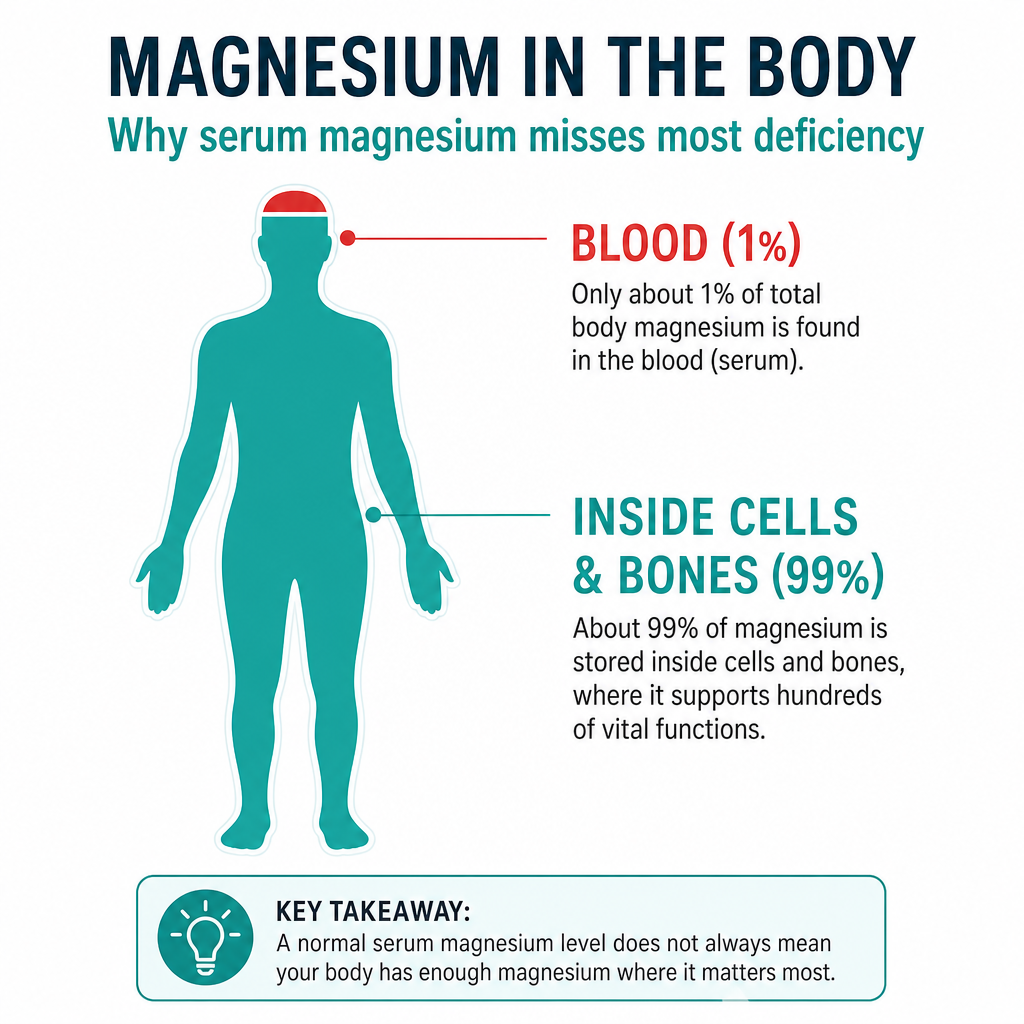
This is one of the most important things to understand.
When a doctor checks "your magnesium," they almost always order serum magnesium.
But only about 1% of the body's magnesium lives in the blood. The other 99% sits inside cells and in bone.
That means:
- Serum magnesium can look "normal" while tissue or intracellular status is suboptimal
- Serum magnesium typically falls only after deficiency is severe and prolonged
- A normal result on this test does not rule out a problem
Additional markers that may help in selected cases include:
- RBC (red blood cell) magnesium — more reflective of intracellular status
- Ionized magnesium — the metabolically active fraction
- 24-hour urinary magnesium — useful for assessing losses
- Magnesium loading tests — research-grade
In a more detailed workup, magnesium can be evaluated using a combination of serum values, clinical context, medications, diet, symptoms, and sometimes additional tests.
If you've been told "your magnesium is fine" based on a basic metabolic panel, that conclusion may be premature.
Real Clinical Case: A Stage 3b CKD Patient Whose Plateau Was Magnesium
Here's a case from my own practice that shows how easily this gets missed.
A woman in her early 60s with stage 3b CKD, well-controlled hypertension, and type 2 diabetes had been "doing everything right":
- Followed a careful low-potassium diet
- Took her ACE inhibitor and metformin reliably
- Kept her blood pressure in range
- Lost weight
- Walked daily
And yet her kidney function continued to slowly slip. She was also struggling with:
- Persistent leg cramps at night
- Restless, poor-quality sleep
- Low energy
- New episodes of atrial fibrillation
- Tension headaches
Her nephrologist had checked a basic metabolic panel. Serum magnesium: 1.8 mg/dL — "normal."
When her plan was reassessed in a comprehensive workup:
- RBC magnesium was clearly low
- She had been on a PPI for years for reflux
- She was on a thiazide diuretic
- Her low-potassium diet had eliminated almost every magnesium-rich food
Her plan was adjusted thoughtfully:
- The PPI was weaned and replaced with root-cause reflux work (a separate but related conversation)
- A well-tolerated, kidney-appropriate form of magnesium was introduced at a low starting dose with close monitoring
- Selected magnesium-rich foods were carefully reintroduced based on her individual labs
- Stress and sleep were addressed in parallel
- Blood pressure medications were re-evaluated
Six months later:
- Night cramps were gone
- Sleep was deeper
- Atrial fibrillation episodes had reduced significantly
- Blood pressure stabilized on a lower medication dose
- The slow decline in her GFR had flattened
- Her energy returned
I'm careful, as always, about how I frame this:
Magnesium repletion didn't "cure" anything. It corrected a foundational deficiency that was quietly making everything else harder. When you remove the load, the system has room to stabilize.
Magnesium doesn't fix CKD. But when a clinically important deficiency is present, correcting it can take one avoidable stressor off the system.
The Counter-Intuitive Risk: Why Self-Supplementing Magnesium in CKD Is Dangerous
Now for the warning that has to live next to all of this.
If you have CKD, magnesium is not something to start on your own at a high dose from the supplement aisle.
When kidney function is reduced, the kidney's ability to excrete excess magnesium is also reduced. That means hypermagnesemia — too much magnesium — becomes a real risk, especially in:
- Stage 4 and 5 CKD
- Patients on dialysis
- Patients taking magnesium-sparing medications
- Anyone using magnesium-containing laxatives or antacids
Severe hypermagnesemia can cause:
- Muscle weakness
- Low blood pressure
- Slow heart rate
- Respiratory depression
- Cardiac arrest (rare but real)
This is one reason clinicians are cautious with magnesium in kidney disease — and why some patients are told to avoid unsupervised supplementation.
The reality is more nuanced:
- Early-stage CKD (1-3a): Often compatible with thoughtful repletion when there is a clear reason.
- Mid-stage CKD (3b): Possible for some patients with careful selection, low doses, and lab monitoring.
- Advanced CKD (4-5): Generally requires physician oversight, individualized assessment, and avoidance of high-dose oral magnesium unless specifically directed.
This is one of the strongest arguments for working with a clinician instead of guessing.
Form Matters: Not All Magnesium Is the Same
If magnesium is recommended for you, the form matters as much as the dose.
The most absorbable, best-tolerated forms include:
- Magnesium glycinate — gentle on the gut, supports sleep
- Magnesium malate — energy support
- Magnesium taurate — cardiovascular focus
- Magnesium L-threonate — best for cognitive support
Forms to generally avoid for repletion:
- Magnesium oxide — poorly absorbed (about 4%), mostly a laxative
- Magnesium citrate at high dose — can cause diarrhea
- Magnesium hydroxide (milk of magnesia) — laxative effect
- High-magnesium antacids — risk of accumulation in CKD
And — as always for any supplement when kidney function is reduced — choose third-party tested products and avoid blends that hide doses or add unnecessary herbs.
Foods That Replenish Magnesium Safely (Even in CKD)
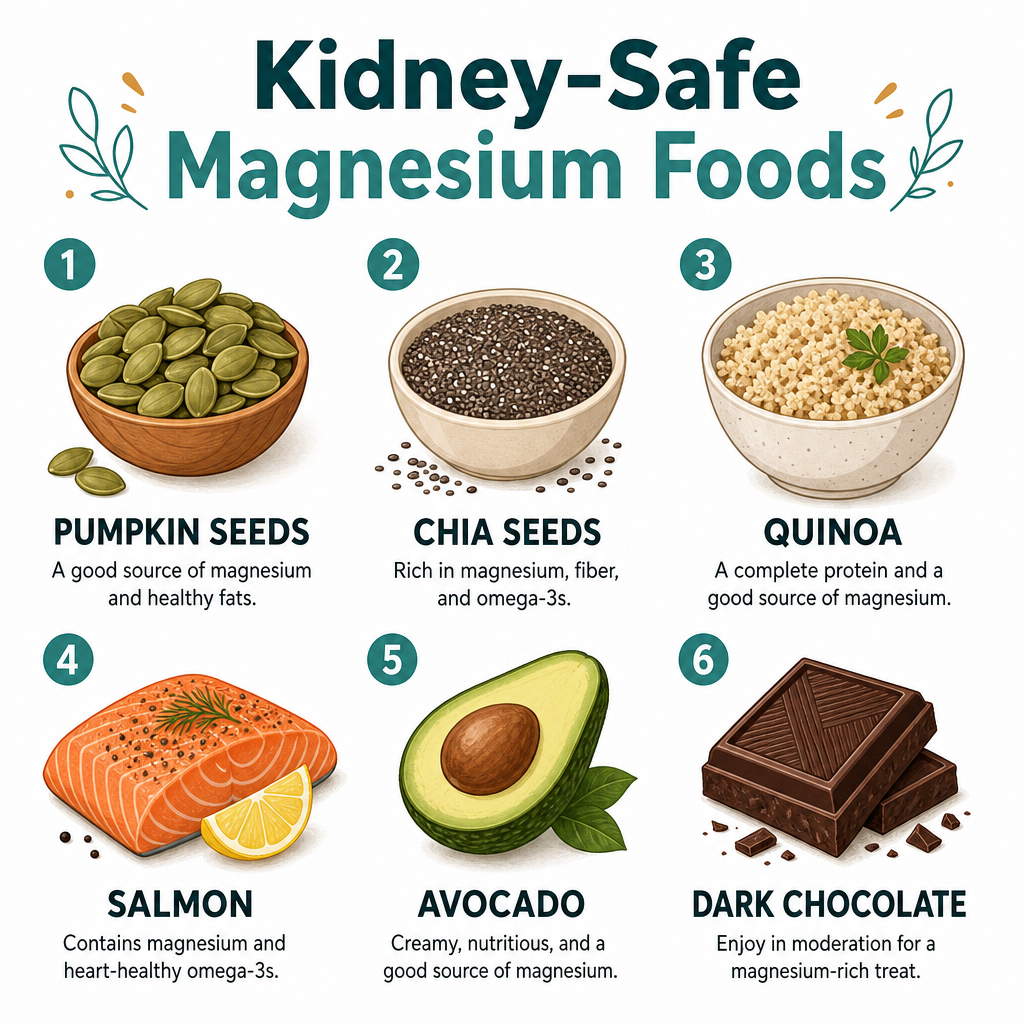
Not every magnesium-rich food is automatically off-limits in CKD. Some can be reintroduced — in modest, individualized portions — once potassium, phosphorus, labs, and medications are reviewed.
Lower-risk, magnesium-supportive choices that often fit a kidney-aware plate include:
- Pumpkin seeds (small portions — also rich in zinc)
- Chia seeds (excellent in moderation)
- Quinoa
- Wild-caught salmon and mackerel
- Avocado (portion-controlled)
- Dark chocolate (85%+ cocoa, small squares)
- Selected leafy greens, in amounts that fit your potassium plan
The right list for you depends on your labs, stage, and medications. There is no universal renal diet.
Working With (Not Against) Your Nephrologist
A note for patients and family members:
You should not arrive at your nephrologist's office with a bottle of magnesium and an argument.
You should arrive with better questions:
- "What is my serum magnesium right now? Has RBC magnesium ever been checked?"
- "How many of my current medications are known magnesium-wasters?"
- "Given my CKD stage, is a low, monitored dose of magnesium appropriate?"
- "Can we look at intracellular and ionized markers instead of just serum?"
Most clinicians respond better to specific, safety-focused questions than to supplement arguments. If you feel dismissed, a second opinion can be useful — especially when symptoms, diet, and medications are not being reviewed together.
Three Key Takeaways
1. Magnesium Status Is Worth Checking in the Right CKD Patients
Low magnesium is common in some CKD populations, especially with diabetes, restrictive diets, PPIs, and diuretics. Advanced CKD can also create the opposite problem — high magnesium — so testing and context matter.
2. The Conventional Kidney Diet, Combined with Common Medications, Drives the Deficiency
Restricting potassium can remove foods rich in magnesium. PPIs, loop diuretics, thiazides, diabetes, and some other medications or conditions can increase risk. The result is not automatic, but it is worth assessing.
3. Repletion Must Be Personalized — Not DIY'd
Magnesium can help when a true deficiency exists, but in CKD it can also accumulate dangerously. The right form, dose, product quality, and lab monitoring matter. Advanced CKD requires real supervision.
Conclusion: The Mineral That Quietly Holds Everything Together
CKD is rarely lost to one big thing. It is usually lost to the slow accumulation of small, unaddressed loads — silent inflammation, mild metabolic dysfunction, unnoticed deficiencies — that, over years, exhaust the kidney's reserve.
Magnesium is one of those loads when it's missing.
It quietly holds together blood pressure regulation, insulin signaling, vascular protection, inflammation control, sleep, mood, and the rhythm of the heart itself. Take it away, and every other intervention has to work harder than it should.
The good news is that magnesium status is measurable and often modifiable. The important step is not self-supplementing — it is asking better questions and matching the plan to your labs.
Ask.
Watch the full interview:
🩺 Ready to find what your conventional workup is missing? Book a Comprehensive Kidney Consult with Dr. Bismah →
📖 Free resources: - Find Your Kidney Root Cause - 7 Super Foods for Kidneys - 21-Day Kidney Function Boost
This article is for educational purposes only and does not constitute medical advice. Magnesium supplementation in CKD requires individualized evaluation — always consult your physician before starting any supplement, especially with reduced kidney function.
Selected References
- Zhan Y, Zhang R, Li G. Effect of magnesium on vascular calcification in chronic kidney disease patients: a systematic review and meta-analysis. Renal Failure. 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC9980397/
- Zaslow SJ, Oliveira-Paula GH, Chen W. Magnesium and Vascular Calcification in Chronic Kidney Disease: Current Insights. International Journal of Molecular Sciences. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC10816532/
- National Kidney Foundation. Vitamins in Chronic Kidney Disease. https://www.kidney.org/kidney-topics/vitamins-chronic-kidney-disease
- Merck Manual. Hypermagnesemia. https://www.merckmanuals.com/home/kidney-and-urinary-tract-disorders/electrolyte-balance/hypermagnesemia-high-level-of-magnesium-in-the-blood